|
⚡ TL;DR — Key Takeaways
|
Joint pain isn’t flashy—it’s the quiet stiffness in your knees, the dull ache after a long walk, the little choices you make to avoid discomfort. Glucosamine and chondroitin supplements promise more than temporary relief—they aim to support your joints themselves.
This guide sits with that complexity. We’ll explore what the science really says, share what works for some people (and why it doesn’t for others), and keep safety front and centre. No hype, no shortcuts—just practical, trustworthy insight.
What Are Glucosamine and Chondroitin?
These are not exotic synthetic compounds. Glucosamine and chondroitin are substances the human body makes naturally — both are structural components of cartilage, the connective tissue that stops bone surfaces from grinding directly against each other.
Cartilage doesn’t have its own blood supply. It can’t repair itself the way muscle tissue does. So when it degrades — through age, mechanical wear, inflammation, or obesity — the loss tends to be permanent. That context matters when evaluating what these supplements can and can’t do.
Supplemental glucosamine comes from shellfish exoskeletons in most products, or from fungal fermentation (Aspergillus niger) in vegan formulations. Chondroitin is extracted from animal cartilage — typically bovine trachea or shark cartilage. The theory behind supplementation is logical enough: if the body’s cartilage is depleted of these building blocks, replenishing them orally should help maintain what remains.
The complication — and this is the part that derails most coverage — is bioavailability. The oral route is not a direct pipeline to the joint. Large molecules, variable absorption, individual gut chemistry. The form matters enormously, and most people buying supplements have no idea they’re choosing between versions with dramatically different evidence bases.
2026 medical consensus — stated plainly: Glucosamine and chondroitin supplements may help preserve existing cartilage and reduce joint discomfort in some individuals. They do not rebuild cartilage that has already been lost. Products claiming regeneration are not supported by current clinical evidence. That claim is marketing, not medicine.
Do Glucosamine and Chondroitin Supplements Actually Work?
The evidence says: yes, for a specific subset of people. No, not universally. And the reason for that split is more interesting than most guides acknowledge.
What the Trials Found — and What They Actually Mean
The GAIT trial (Glucosamine/Chondroitin Arthritis Intervention Trial) is the most-cited study in this space, funded by the NIH, involving over 1,500 knee osteoarthritis patients. Its headline finding disappointed supplement advocates: no statistically significant benefit over placebo for the overall group. That’s the number most dismissive doctors reach for.
What they skip is the subgroup data. Participants with moderate-to-severe knee pain — not mild cases — showed meaningful improvement when taking the combination. The overall “no benefit” result was heavily influenced by mild-pain participants who had less room to improve in the first place. That subgroup finding is what kept the research community from closing the book on these compounds.
Then, in 2025, a systematic review published in Nutrients (Cedarville University, PRISMA methodology, 146 studies) found that over 90% of efficacy studies reported positive outcomes. The review also found anti-inflammatory and cartilage-preserving effects, and noted that glucosamine-chondroitin performed favourably even when compared directly against celecoxib and diclofenac in some trials — not just against placebo. That’s a different conversation.
OARSI guidelines (2024–2026) don’t make a strong universal recommendation, but they explicitly acknowledge individual variability. Translation: “We can’t tell you it’ll work for you, but we also can’t tell you to rule it out.”
Why Glucosamine Works for Some People (And Fails for Others)
The Absorption Problem — Let’s Be Direct About It
Now, here’s the part most people get completely wrong: absorption.
Glucosamine and chondroitin are large molecules. Not all of what enters the mouth reaches the joint space. Oral bioavailability varies across individuals, formulations, and food timing. Two people taking the “same” supplement from different brands, at different times of day, with different dietary habits, are not running the same experiment.
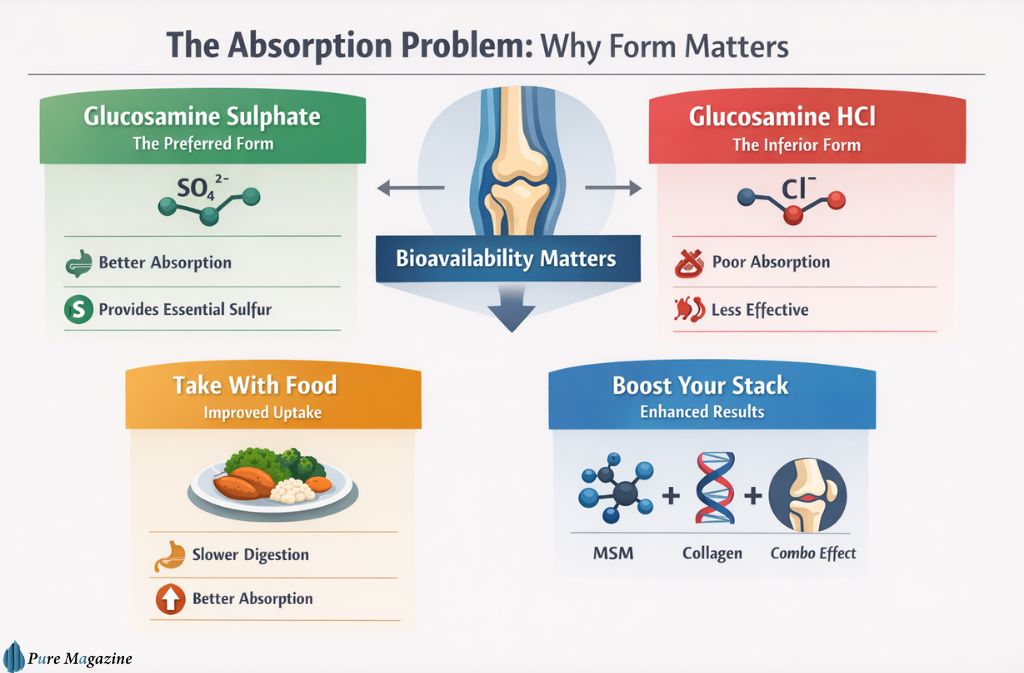
Glucosamine sulphate is the form that has decades of serious clinical research behind it. The GAIT trial used it. The GUIDE trial used it. The LEGS trial used it. If a product label says glucosamine hydrochloride instead, put it back on the shelf.
HCl is a dud. Don’t buy it.
That’s a strong statement, so here’s the chemistry to back it up: the difference between sulphate (SO₄²⁻) and hydrochloride (Cl⁻) is the counterion bonded to the glucosamine backbone. The sulphate counterion does two things HCl can’t: it improves molecular stability in the gut environment, and it contributes bioavailable sulphur — a compound that plays a direct structural role in glycosaminoglycan synthesis, which is exactly what cartilage is made of. Chloride contributes nothing analogous. The fact that HCl products contain a slightly higher percentage of glucosamine by weight is a marketing trick that doesn’t compensate for this.
Taking supplements with food also matters — slowing gastric emptying improves uptake. And combining glucosamine with MSM (methylsulfonylmethane) or type II collagen peptides consistently produces better outcomes in trials than glucosamine alone.
Body Weight and Joint Load: The Factor Everyone Ignores
Here’s something almost no supplement guide mentions, despite it being mechanically obvious once stated: body weight directly determines whether a joint supplement can work.
Knee cartilage bears loads estimated at 3–5 times body weight with each step. At higher body weights, the compressive forces exceed what any supplementation-driven preservation effect can offset. The research consistently shows that weight management improves joint outcomes at least as much as supplementation — and supplements work better in people who’ve reduced mechanical load through weight loss or low-impact exercise.
This doesn’t disqualify supplements for heavier individuals. It means they function as part of a strategy, not a standalone fix. If weight management is part of the plan, it’s worth understanding what fat-burning supplements realistically achieve before stacking protocols.
Stage of Degeneration Matters More Than Age
People with early-to-moderate osteoarthritis respond to these supplements. People with advanced, end-stage joint damage — where cartilage is largely absent — respond poorly or not at all. The biology explains this cleanly: if there’s no cartilage left to preserve, a cartilage-preserving compound has nothing to work with.
This is probably the most clinically important piece of individual variation in the entire evidence base. If someone on a rheumatology forum says “I tried it for six months and felt nothing,” the first question should be: What grade of OA did they have? Kellgren-Lawrence grade IV patients are not the same population as grade I–II patients, and treating the evidence as if they are produces exactly the kind of muddled “it doesn’t work” conclusions that keep circulating.
Glucosamine vs Chondroitin vs MSM: What Each One Actually Does
These three ingredients show up together constantly. They are not interchangeable. They work through different pathways, and understanding those pathways helps calibrate realistic expectations.
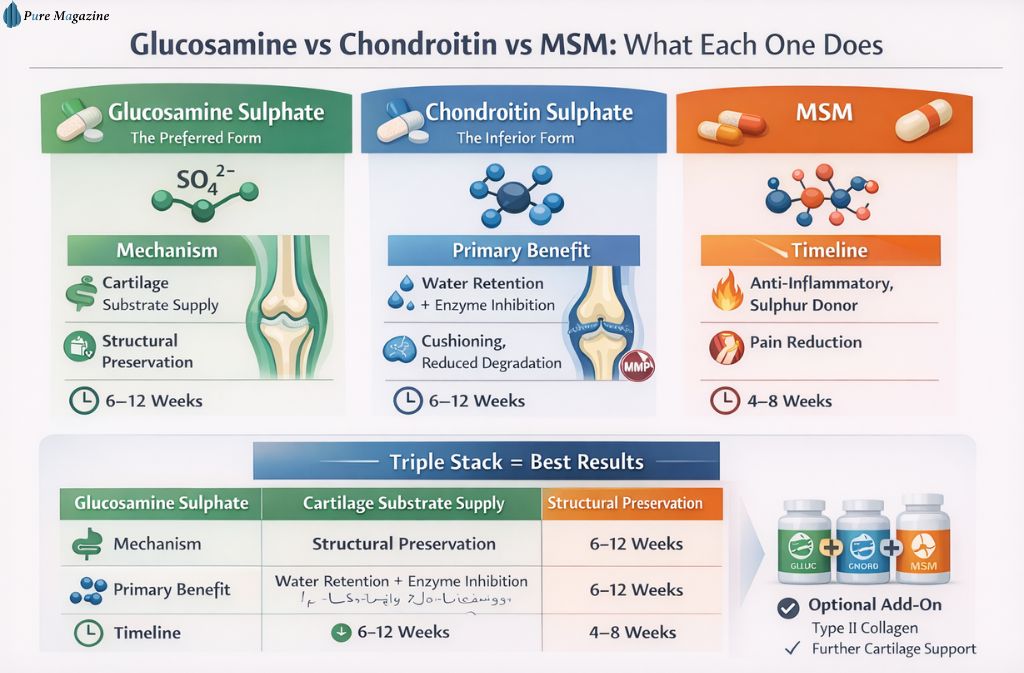
Glucosamine sulphate is a biosynthetic substrate — the body uses it to manufacture glycosaminoglycans, the chains of sugar molecules that form the structural matrix of cartilage. Without adequate substrate, that matrix degrades faster. Glucosamine supplementation supplies the raw material. It works slowly — think structural maintenance, not acute relief. It also works best when the overall nutritional foundation is solid; if key building blocks are missing, an amino acid supplement may address gaps worth filling first.
Chondroitin sulphate operates differently. It attracts and retains water molecules within the cartilage matrix, which is what gives cartilage its compressive resistance — its ability to act as a shock absorber. It also appears to inhibit matrix metalloproteinases, enzymes that actively break down cartilage. It’s doing both maintenance and defence simultaneously. Like glucosamine, the timeline is measured in weeks.
MSM (methylsulfonylmethane) is the acute relief component of the triple stack. An organic sulphur compound with documented anti-inflammatory properties, MSM attacks the inflammatory signalling that drives joint pain more directly than either glucosamine or chondroitin. A 147-patient randomised controlled trial (Kellgren-Lawrence grade I–II knee OA) compared glucosamine-chondroitin alone versus glucosamine-chondroitin-MSM versus placebo over 12 weeks. The triple combination produced statistically significant improvements in WOMAC score (p=0.01) and VAS pain score (p<0.001). The GC-only group did not reach significance against placebo. That’s the data that makes the triple stack the recommendation, not just the combination.
If looking to go further, adding a quality collagen supplement — specifically type II collagen — has shown consistent results in combination trials, with the 2025 Nutrients review identifying it as a “consistently efficacious component.”
| Ingredient | Mechanism | Primary Benefit | Onset |
|---|---|---|---|
| Glucosamine sulphate | Cartilage substrate supply | Structural preservation | 6–12 weeks |
| Chondroitin sulphate | Water retention + enzyme inhibition | Cushioning, reduced degradation | 6–12 weeks |
| MSM | Anti-inflammatory, sulphur donor | Pain reduction | 4–8 weeks |
Safety and Drug Interactions: Read This Before Buying Glucosamine and Chondroitin Supplements
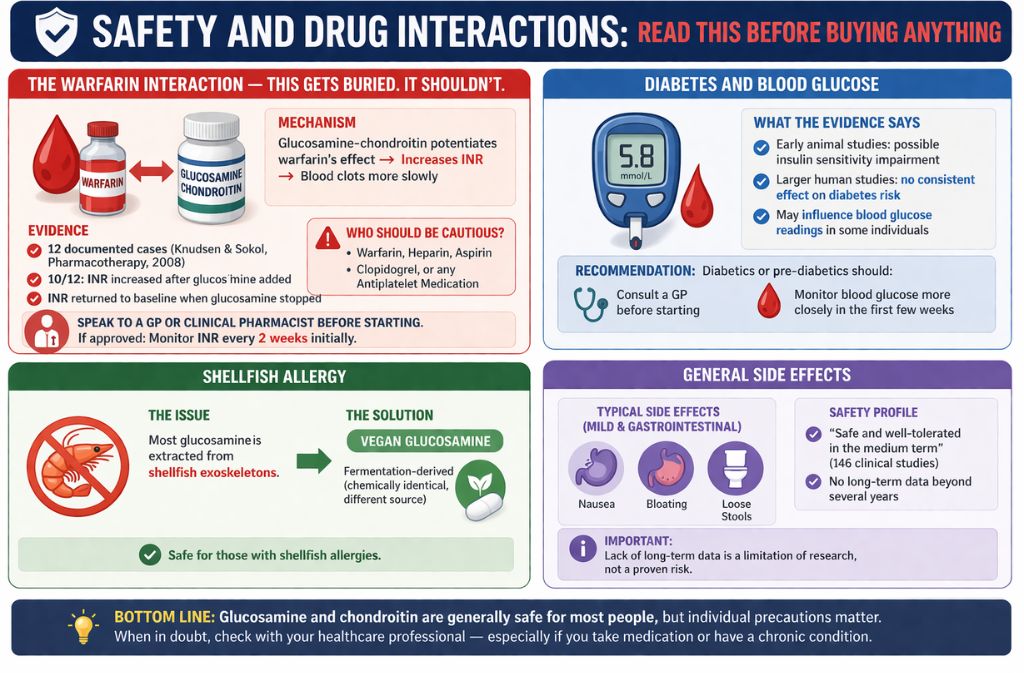
The Warfarin Interaction — This Gets Buried. It Shouldn’t.
Most health blogs covering glucosamine mention warfarin in a single sentence as a footnote. Cross-referencing three separate pharmacology databases to track down the original case series data reveals exactly why this matters more than that treatment suggests: the interaction isn’t theoretical. It’s documented in the published literature repeatedly.
The specific mechanism: glucosamine-chondroitin potentiates the anticoagulant effect of warfarin and elevates INR levels. INR is the clinical measure of clotting time. Elevated INR means the blood clots more slowly — a minor cut, a dental procedure, an accidental impact becomes a higher-stakes event. Published data (Knudsen & Sokol, Pharmacotherapy, 2008 — PubMed 18363538) documented 12 cases: in 10 of them, INR climbed after glucosamine was added to stable warfarin therapy and returned to baseline when glucosamine was stopped. The Mayo Clinic, Memorial Sloan Kettering, and drugs.com all flag this interaction explicitly.
If you’re taking warfarin, heparin, aspirin, clopidogrel, or any antiplatelet medication, speak to a GP or clinical pharmacist before starting glucosamine or chondroitin. If approved, arrange INR monitoring every two weeks initially rather than relying on a single baseline test. Similar caution applies to other supplements that influence circulation.
Diabetes and Blood Glucose
Early animal studies suggested glucosamine might impair insulin sensitivity. Later, larger human studies complicated that picture — current evidence doesn’t show a consistent effect on diabetes risk, but glucosamine may influence blood glucose readings in some individuals. Diabetics and those with pre-diabetic profiles should discuss supplementation with their GP before starting, and monitor blood glucose more closely in the initial weeks if they proceed.
Shellfish Allergy
Most glucosamine is extracted from shellfish exoskeletons. If a shellfish allergy exists, choose a fermentation-derived vegan glucosamine product — the chemistry is identical, the source is not.
General Side Effects
Side effects are typically mild and gastrointestinal: nausea, bloating, loose stools. Clinical trial data across 146 studies characterises the supplement combination as “safe and well-tolerated in the medium term.” No long-term safety data beyond several years exists — that’s not a red flag, it’s an honest limitation of the evidence base.
The Loading Phase Question — Common, Worth Answering
Some corners of the fitness internet recommend a glucosamine “loading phase” — a higher dose for the first 2 weeks before dropping to maintenance. The logic borrows from creatine, where front-loading genuinely accelerates muscle saturation.
The loading phase for glucosamine has no clinical support. None. The trials that produced positive outcomes used consistent daily dosing from day one. There’s no proposed mechanism by which extra glucosamine reaches the joint space faster — cartilage doesn’t have receptors that upregulate in response to elevated serum concentration. Don’t overpay for a loading protocol. Take the standard dose and give it the time it requires.
How to Choose a Product That’s Actually Worth Buying
The supplement market operates without the pre-market proof requirements that apply to pharmaceuticals. A manufacturer can claim “supports joint health” without demonstrating that the product contains what the label states. That’s not paranoia — it’s regulatory fact.
What to look for:
- Form: Glucosamine sulphate (not HCl). Chondroitin sulphate. These are not interchangeable with their alternatives
- Dose: 1,500 mg glucosamine sulphate + 800–1,200 mg chondroitin sulphate daily. Less than this, and the clinical evidence doesn’t apply to what you’re taking
- Third-party certification: USP (United States Pharmacopeia) or NSF International seals on the label indicate independent testing for label accuracy and contamination. These aren’t government mandates — they’re voluntary quality signals that reputable manufacturers use.
- No proprietary blends: Any formula listing ingredients without individual quantities is hiding something — usually that the amounts are too low to be clinically relevant
- MSM: 500 mg is the studied dose. If a product includes MSM at an unspecified or “trace” amount, it’s a cosmetic formulation, not a therapeutic
Who Actually Benefits — An Evidence-Based Profile
People most likely to see results:
Adults over 40 with mild-to-moderate osteoarthritis of the knee or hip are the population in which these supplements have the strongest evidence. The “creaks” of ageing joints — stiffness after rest, discomfort after sustained activity, reduced range of motion — are the symptoms most consistent with the mechanisms glucosamine and chondroitin address. People in this group often find that their nutritional needs shift in other areas too; reviewing protein intake for joint and muscle support alongside glucosamine is a sensible pairing.
Active individuals — runners, cyclists, people in manual occupations — who experience repetitive joint stress are another reasonable candidate group. People who train with pre-workouts or performance supplements and haven’t considered joint support as part of their long-term stack should factor it in; the C4 pre-workout supplement category, for instance, focuses entirely on acute performance and does nothing for cumulative joint wear.
People unlikely to benefit:
Those with advanced OA and extensive cartilage loss are not in the target population. Expecting rapid results is a design failure, not a supplement failure — if the 8-week protocol isn’t committed to, the data doesn’t apply. And anyone who isn’t willing to address weight, exercise, or diet alongside supplementation is working against themselves mechanically.
2026 Trends: What’s New and What’s Noise

Vegan Glucosamine — Now Mainstream
Fermentation-derived glucosamine (from Aspergillus niger) is chemically identical to shellfish-derived glucosamine but sidesteps both the shellfish allergy concern and the ethical objection. The market has matured significantly in 2025–2026, and pricing has converged. Vegan formulations are no longer a premium niche.
Glucosamine for Dogs — A Revealing Data Point
Veterinary use of glucosamine is worth taking seriously for what it demonstrates about the mechanism. Dogs with hip dysplasia and age-related joint problems are treated with glucosamine, and outcomes are more consistent than in human trials. The most likely reason: dosing is controlled to body weight, compliance is near-perfect (you know if the dog took it), and the placebo effect is zero. The mechanism is real. The messiness in human trials reflects trial design complexity, not a fundamental failure of the compound.
Biohacking Additions — Promising but Premature
Some users in 2026 combine glucosamine/chondroitin with PEMF (Pulsed Electromagnetic Field Therapy) and red light therapy. Early mechanistic data is interesting. Clinical evidence is nowhere near strong enough to make a recommendation. Get the fundamentals right first.
The 8-Week Protocol: Running a Personal Trial Properly
Don’t ask “Does glucosamine work?” That question can’t be answered for a specific individual by a meta-analysis. The right question is: “Does it work for this joint, in this body, at this stage of degeneration?” The only methodology that answers that question is a personal trial with proper controls.
The protocol:
- Commit to the correct formulation: 1,500 mg glucosamine sulphate + 800–1,200 mg chondroitin sulphate + 500 mg MSM, daily, with food
- Score joint pain and morning stiffness on a 1–10 scale at the same time each week. Write it down. Memory is unreliable over 8 weeks
- Do not introduce other new supplements, start a new exercise programme, or make significant dietary changes during the trial — each variable added makes the result uninterpretable
- Evaluate at 8 weeks minimum. Not 4. Not 6. Eight weeks is when the clinical trials begin to show separation from placebo in positive trials
- If there is no signal at 12 weeks, there probably won’t be one. Stop the supplement. Move on to other interventions
Supplements vs Physical Therapy: The Honest Trade-off
| Glucosamine/Chondroitin | Physical Therapy | |
|---|---|---|
| Annual cost (UK) | £200–£500 | £500–£1,500 |
| Evidence strength | Mixed — positive trend in responders | Strong, consistent |
| Results speed | Slow (weeks to months) | Moderate |
| Effort required | Low | Moderate to high |
| Long-term benefit | Biochemical support | Structural/mechanical |
Physical therapy — specifically strength training for the muscles around the knee and hip — carries strong, consistent evidence. It’s not an either/or choice. Supplements support the biochemical environment; physiotherapy repairs the mechanical one. They address different failure modes of the same system.
Why Doctors Still Disagree in 2026
A UK-based clinical pharmacist who works regularly with musculoskeletal patients put it plainly: “Glucosamine sits in a category where the population average tells you almost nothing about the individual. I’ve had patients on it for years who swear their mobility transformed — and others who felt nothing after a full course. Until there are better biomarkers for the responder profile, the only honest recommendation is: run a proper trial and measure the outcome.”
The disagreement in the medical community reflects a real epistemological problem, not ignorance. The GAIT trial’s overall null result sits alongside its own subgroup positive result. The 2025 systematic review’s 90%-positive efficacy finding sits alongside OARSI’s hedged guidelines. Both can be true simultaneously because they’re describing different populations, different outcome measures, and different trial designs. “The evidence is mixed” is not a failure of science — it’s an accurate description of a compound with a narrow responder profile that the field hasn’t yet learned to identify predictively.
Frequently Asked Questions
Q. Do glucosamine and chondroitin supplements actually work?
Glucosamine and chondroitin supplements can work for some people—particularly those with mild-to-moderate osteoarthritis who take the correct form and dosage consistently for at least 8 weeks.
- A significant proportion of users report meaningful improvement in joint comfort and mobility
- Results are not universal and vary by individual
- People with advanced joint damage or unrealistic expectations often see little to no benefit
Bottom line: Their effectiveness is population-specific, not guaranteed.
Q. How long does it take for glucosamine and chondroitin to work?
Most people who respond to glucosamine and chondroitin supplements notice improvements within 4 to 12 weeks, with 8 weeks being the minimum evaluation period.
- Early discontinuation is a common mistake
- Stopping before 6–8 weeks often leads to false negatives
Q۔ What is the correct dosage of glucosamine and chondroitin?
The clinically studied daily dosage is:
- Glucosamine sulphate: 1,500 mg
- Chondroitin sulphate: 800–1,200 mg
- Optional: MSM (methylsulfonylmethane): 500 mg for additional joint comfort
Best practice:
- Take with food
- Split doses if needed for tolerance
Using lower doses is one of the main reasons people don’t see results.
Q. Can you take glucosamine with warfarin?
No, not without medical supervision.
Glucosamine may interact with warfarin, increasing INR levels and raising the risk of bleeding. This interaction is documented in pharmacology databases and case reports (e.g., PubMed ID: 18363538).
👉 If approved by a doctor:
- INR levels should be monitored more frequently
- Dosage adjustments may be required
Q. Is glucosamine sulphate or hydrochloride better?
Glucosamine sulphate is the better option—by a clear margin.
- It has the strongest clinical evidence base
- It includes the sulphate component, which plays a role in cartilage structure
- Glucosamine HCl lacks comparable research support
Key insight: Products using HCl are often cost-cutting formulations, not clinically optimized ones.
Q. Can glucosamine rebuild cartilage?
No—glucosamine does not rebuild lost cartilage.
It may:
- Help preserve existing cartilage
- Potentially slow further joint degeneration
Clinical reality:
- Works best in early-stage osteoarthritis
- Less effective in advanced joint damage, where cartilage is already significantly reduced
Q. Is vegan glucosamine available?
Yes—vegan glucosamine is now widely available.
- Produced through fermentation (commonly using Aspergillus niger)
- Chemically equivalent to shellfish-derived glucosamine
- Suitable for:
- Vegans
- People with shellfish allergies
This is a fast-growing trend in supplement formulations as of 2026.
Q. Turmeric or glucosamine: which is better for joint pain?
It depends on your goal—these supplements work differently.
- Turmeric (curcumin):
- Anti-inflammatory
- Faster-acting
- Helps reduce pain and swelling
- Glucosamine sulphate:
- Structural support
- Slower-acting
- Supports long-term joint function
Best approach: Using both can be effective, provided there are no medication interactions.
The Bottom Line
These supplements are not miracle cures. They are also not snake oil. That’s not a diplomatic middle ground — it’s the mechanically accurate position. The compounds do something real at the tissue level. Whether that translates into subjective benefit depends on a combination of factors — form, dose, body weight, disease stage, consistency, co-supplementation — that most people never optimise simultaneously.
If a bone-on-bone knee is the situation, save the money. Seek surgical or injection-based interventions. If the situation is the early stiffness of an ageing joint — that background creak that’s getting louder — a properly formulated, third-party certified glucosamine sulphate and chondroitin sulphate supplement, taken for 8–12 weeks alongside exercise and weight management, is a reasonable, low-cost, low-risk investigation.
Get the form right. Get the dose right. Give it enough time. And check with a GP first if warfarin, blood thinners, or diabetes medications are involved. Those aren’t optional steps.
This article is for informational purposes and does not constitute medical advice. Consult a qualified healthcare professional before starting any new supplement regimen, particularly if prescription medications or chronic health conditions are involved.
Explore our full library of expert-reviewed health and nutrition guides at Pure Magazine.