Nobody talks about hormones until something goes wrong. Then suddenly everything is a symptom — the fatigue, the weight that won’t shift, the mood that turns on a dime, the skin that’s staging a revolt. And the supplement aisle responds accordingly, stacking shelves with “hormone balance” blends that list twelve ingredients, dose none of them properly, and charge you forty pounds for the privilege.
Here’s what that aisle won’t tell you: most hormonal imbalances aren’t a single-hormone problem. It’s a systems problem—insulin resistance feeding into elevated androgens. Cortisol is chronically elevated and suppresses progesterone. Liver detox pathways are sluggish enough that estrogen recirculates instead of clearing. Fix the system, and the hormones often sort themselves out. Chase individual hormones with random supplements, and you’ll be cycling through products indefinitely.
This guide covers what actually works, why it works, and what the research says — without the usual hedging that makes most hormone content useless.
Quick Reference
| Nutrient | What It Does | Best For | Daily Dose |
|---|---|---|---|
| Vitamin D | Acts as prohormone | PCOS, fatigue, cycle irregularity | 1000–4000 IU |
| Vitamin B6 | Supports progesterone synthesis | PMS, mood instability | 10–50 mg |
| Magnesium | Lowers cortisol via GABA | Stress, poor sleep, PMS | 200–400 mg |
| Omega-3s | Improves hormone receptor sensitivity | Acne, PCOS, inflammation | 1–3g EPA/DHA |
| Zinc | Enables T4→T3 thyroid conversion | Low energy, slow metabolism | 15–30 mg |
| DIM | Clears excess estrogen | Estrogen dominance, bloating | 100–200 mg |
| Inositol | Corrects insulin signalling | PCOS, hormonal acne | 2–4g |
What “Hormone-Regulating Vitamins” Actually Means
These aren’t hormones. They’re cofactors — raw materials your body needs to produce hormones, respond to them at the receptor level, and clear them once they’ve done their job.
That third part — clearance — is where most hormone content falls flat. A lot of people are not producing too much estrogen. They’re failing to eliminate it efficiently. The liver processes estrogen in two phases: breakdown and excretion. When either phase is compromised by poor diet, alcohol, or specific nutrient gaps, estrogen gets reabsorbed through the gut and recirculates. The result looks like estrogen dominance even when production is normal.
That distinction changes everything about which supplements are actually relevant to your situation.
Vitamin D: More Hormone Than Vitamin
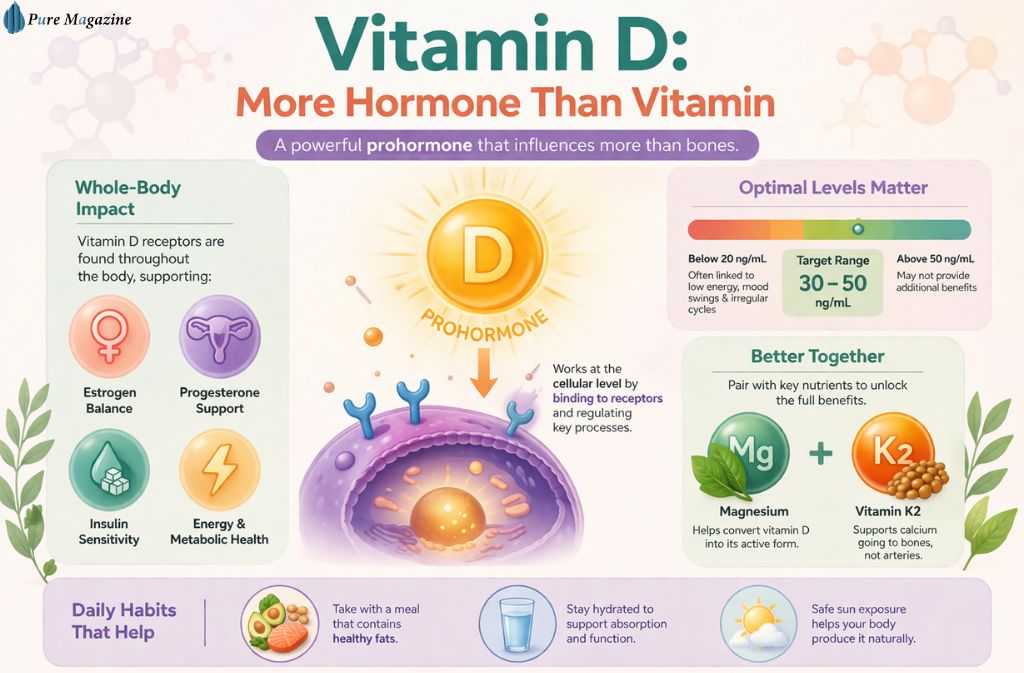
The reclassification of vitamin D as a prohormone isn’t semantic. It binds to receptors throughout the body — not just in bones — and directly influences estrogen, progesterone, and insulin signalling. Low levels don’t just affect bone density. They show up as fatigue, irregular cycles, worsening PCOS symptoms, and metabolic sluggishness.
A 2019 meta-analysis in Nutrients found consistent associations between vitamin D deficiency and PCOS severity — particularly around insulin resistance and ovulatory dysfunction. This isn’t fringe research. It’s been replicated enough times to be considered settled.
Test before you supplement. Target range is 30–50 ng/mL. Anything below 20 ng/mL and you’ll notice it — usually as fatigue and mood instability that nothing else seems to fix. Take it with a fat-containing meal. Pair it with magnesium, which is required for vitamin D conversion, and K2, which prevents the calcium that vitamin D mobilises from depositing in arterial walls instead of bone.
Taking vitamin D without K2 isn’t dangerous in the short term. Over the years, it may contribute to arterial stiffness. It’s an easy fix — take them together.
B Vitamins: The Overlooked Mood and Cycle Connection
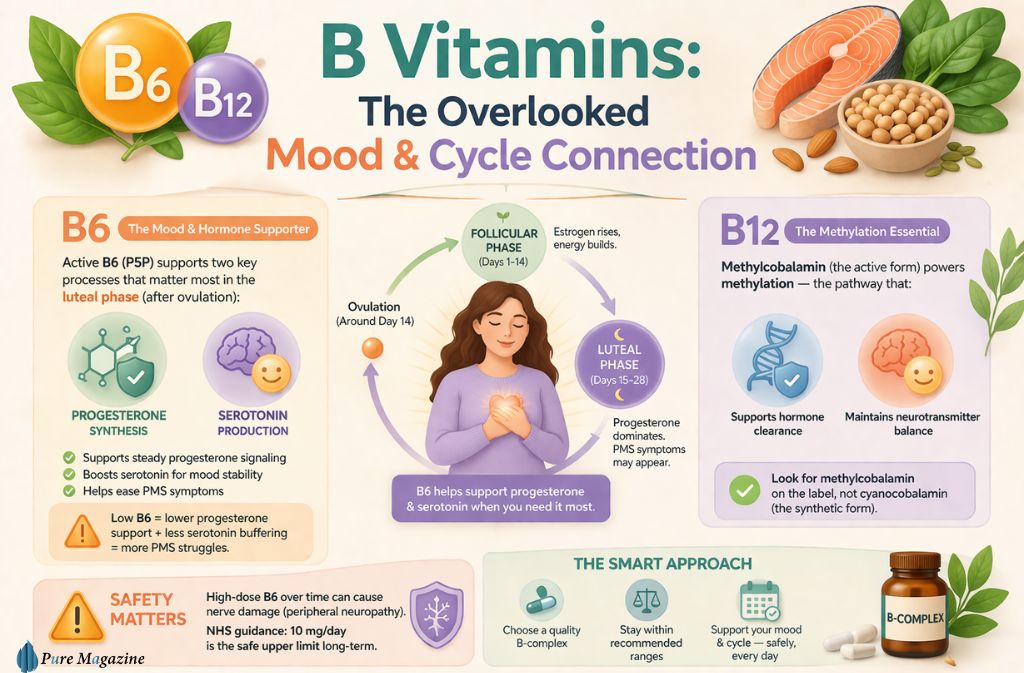
B6 in its active P5P form sits at the intersection of progesterone synthesis and serotonin production. Both matter for the luteal phase — the two weeks after ovulation, where PMS symptoms are most likely to surface. Low B6 means lower progesterone signalling and less serotonin buffering. The result is mood instability, irritability, and the kind of premenstrual experience that makes the second half of the cycle genuinely difficult.
B12 as methylcobalamin — not the synthetic cyanocobalamin found in cheaper supplements — supports the methylation pathways that underpin hormone clearance and neurotransmitter balance. If you’re taking a multivitamin and wondering whether it’s actually doing anything, checking the form of B12 it contains is a reasonable starting point.
One important limit: high-dose B6 sustained over months carries documented peripheral neuropathy risk. The NHS guidance on B vitamins puts the safe upper limit at 10mg daily for long-term use. A quality B-complex within normal ranges is safer than isolated high-dose B6.
Magnesium: The One Most People Are Actually Deficient In

Magnesium deficiency is not a niche problem. Modern diets — heavily processed, low in leafy greens, high in refined carbohydrates — deplete it consistently. And when magnesium is low, the knock-on effects hit multiple hormonal systems simultaneously: cortisol rises because GABA activity drops, sleep quality deteriorates, insulin sensitivity worsens, and PMS intensifies.
Research published in Magnesium Research confirmed what most clinicians working in this space already suspected — chelated forms absorb meaningfully better than oxide. Magnesium oxide is what you’ll find in most cheap supplements and many multivitamins. It functions primarily as a laxative. Magnesium bisglycinate or glycinate is what you actually want for nervous system and hormonal applications.
200–400 mg in the evening is the standard approach. The combination of magnesium and B6 has specific evidence for PMS relief — better together than either alone. If you’re dealing with stress-driven hormonal disruption, this pairing is the most practical starting point before anything more targeted.
Omega-3s: Cell Membranes and Hormone Sensitivity
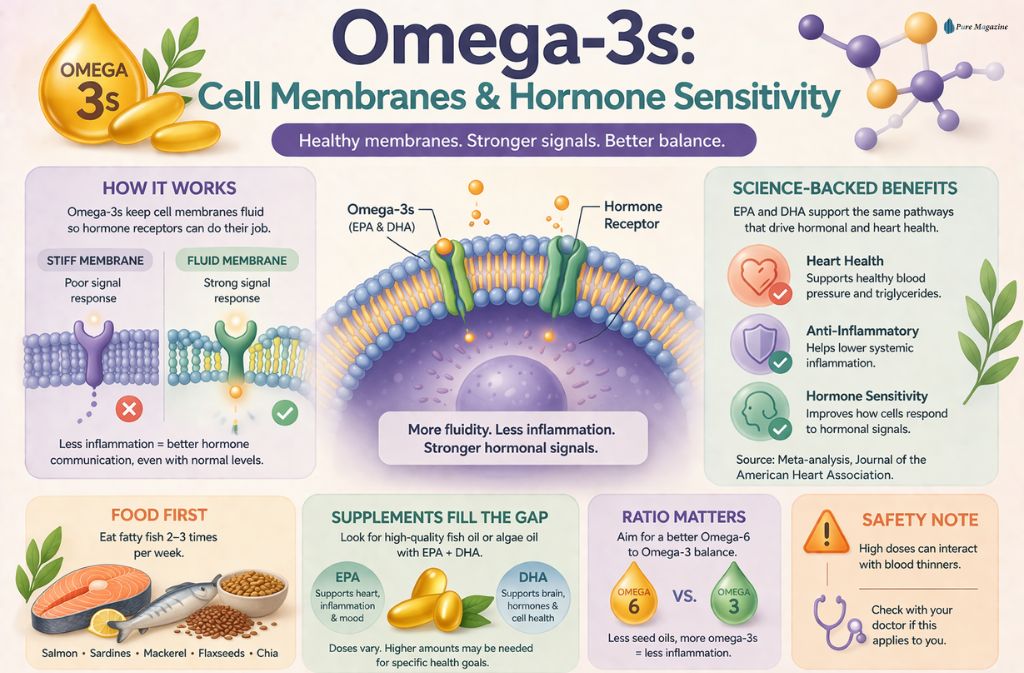
Omega-3 fatty acids don’t produce hormones. What they do is maintain the cell membrane fluidity that determines how efficiently hormone receptors function. A cell membrane that’s stiff and inflammatory responds poorly to hormonal signals — even when those hormones are present in normal amounts. This is partly why omega-3 deficiency shows up as hormonal symptoms despite apparently normal hormone levels on a blood panel.
A large meta-analysis in the Journal of the American Heart Association confirmed cardiovascular and anti-inflammatory benefits from EPA and DHA supplementation — the mechanisms that matter for hormonal signalling run through the same inflammatory pathways.
Fatty fish, two to three times weekly, is the foundation. Supplementation fills the gap when that’s not consistent. Reducing omega-6 intake from processed seed oils matters alongside increasing omega-3 — the ratio between them influences systemic inflammation as much as absolute omega-3 levels do. Higher doses interact with blood thinners, so flag it with a doctor if that’s relevant.
Zinc and Selenium: The Thyroid Pair Nobody Talks About
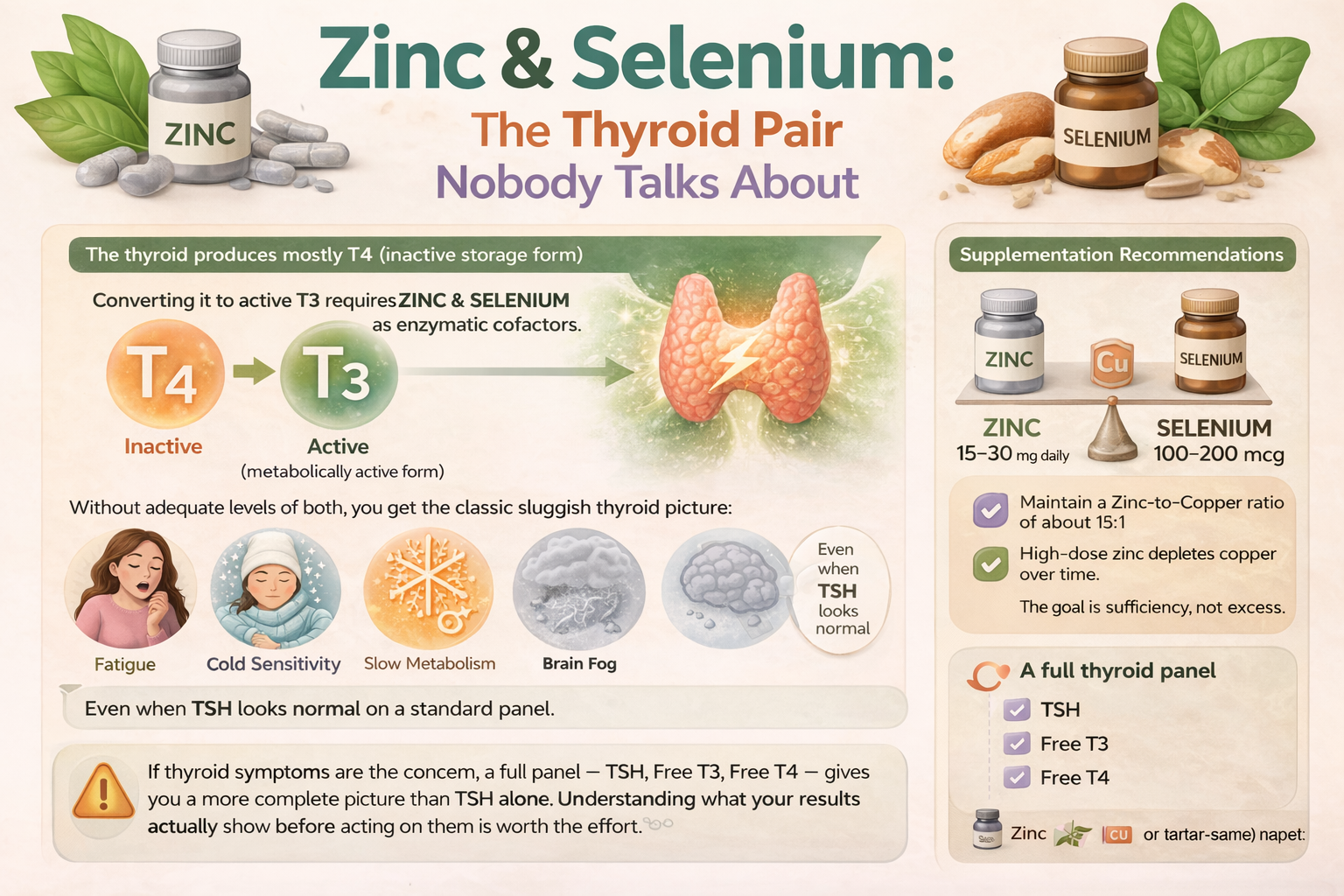

The thyroid produces mostly T4, an inactive storage form. Converting it to active T3 requires zinc and selenium as enzymatic cofactors. Without adequate levels of both, you get the classic sluggish thyroid picture: fatigue, cold sensitivity, slow metabolism, brain fog — even when TSH looks normal on a standard panel, because the conversion problem sits downstream of what TSH measures.
A study in the Journal of the American College of Nutrition found that correcting both deficiencies restored normal thyroid hormone conversion in people who had been symptomatic despite normal-looking thyroid function tests.
Zinc at 15–30 mg daily. Selenium at 100–200 mcg. The zinc-to-copper ratio matters for long-term use — sustained zinc supplementation depletes copper, so staying around a 15:1 ratio is worth tracking. Neither mineral benefits from megadosing. The goal is sufficiency, not excess.
If thyroid symptoms are the concern, a full panel — TSH, free T3, free T4 — gives you a more complete picture than TSH alone. Understanding what your results actually show before acting on them is worth the effort.
DIM and Calcium D-Glucarate: The Clearance Piece
DIM — diindolylmethane, derived from cruciferous vegetables — supports phase one liver detox and shifts estrogen metabolism toward less potent, more easily cleared metabolites. Calcium D-glucarate inhibits the enzyme that allows estrogen to be reabsorbed in the gut, supporting phase two elimination. Together they address clearance rather than production, which, as mentioned at the outset, is often the actual problem.
100–200 mg DIM daily is the working range. Supporting it with adequate water intake and dietary fibre helps the elimination pathway complete the job. Without fibre, cleared estrogen has fewer routes out. It’s a system — each part depends on the others functioning.
Inositol: The PCOS Game-Changer

If there’s one supplement in this list with a genuinely strong evidence base for a specific condition, it’s inositol for PCOS. Not strong in a “promising early research” way. Strong in a “multiple randomised controlled trials with consistent outcomes” way.
Inositol improves insulin sensitivity — and through that mechanism, often restores ovulation in women with anovulatory PCOS, because the insulin dysfunction driving the condition is addressed upstream rather than managed symptomatically. A 2019 clinical review in the International Journal of Endocrinology confirmed that the 40:1 myo to D-chiro-inositol ratio outperformed D-chiro-inositol alone across multiple PCOS outcomes, including ovulation rate, androgen levels, and metabolic markers.
The ratio matters. Most products that simply say “inositol” without specifying the ratio are using D-chiro alone or an unspecified blend. 2–4g daily of the 40:1 formulation, combined with vitamin D and magnesium, addresses the insulin, inflammation, and cortisol arms of PCOS more comprehensively than any single-nutrient approach.
Fix insulin, and hormones often normalise downstream. It’s not guaranteed — but it’s the most direct lever available without prescription intervention.
Cycle Syncing: Timing Nutrients to the Cycle
Hormone needs aren’t static across the month. In the follicular phase — roughly days one through fourteen — estrogen is rising. B-complex vitamins and vitamin D are most relevant here, supporting the metabolic activity that peaks around ovulation.
In the luteal phase — days fifteen through twenty-eight — progesterone should be dominant. Magnesium and B6 become the priority, managing the cortisol and mood instability that tend to surface when progesterone support is inadequate.
Cycle syncing isn’t mandatory. But it reflects how the body actually works — and timing nutrients accordingly gets more from them than treating the month as a flat, undifferentiated stretch.
When Supplements Aren’t Enough
PCOS with significant insulin resistance, thyroid conditions beyond nutrient deficiency, perimenopause, and post-pregnancy hormonal disruption often require clinical management rather than self-directed supplementation. Nutrients support a functioning system — they don’t override a system that needs medical attention.
For older adults navigating hormonal changes alongside age-related muscle loss and metabolic shifts, the interaction between protein intake and hormonal health is worth understanding as a connected picture. These systems don’t operate independently, and addressing one without the other produces incomplete results.
Collagen is another nutrient that intersects with hormonal health in ways that aren’t always obvious — whether collagen supplements actually do what they claim is a reasonable question to have answered before adding it to an already complex protocol.
Safety: What to Actually Watch
High-dose B6 sustained over months — peripheral neuropathy risk, documented and real. Omega-3s at therapeutic doses interact with anticoagulants. Long-term zinc supplementation depletes copper. Vitex (chaste tree berry) can worsen certain hormonal patterns if used in the wrong context — it’s not universally beneficial despite its reputation.
Generic “hormone balance blends” that combine ten active compounds without transparent dosing are worth skipping. You can’t assess what you’re actually getting, you can’t adjust individual components, and you have no way of knowing which ingredient, if any, is doing something useful.
Practical Starting Points
Test before supplementing where possible — vitamin D, B12, thyroid markers, and iron at a minimum. Reduce ultra-processed foods and refined carbohydrates, which drive the insulin dysfunction underlying many hormonal issues more directly than any supplement can counteract. Prioritise sleep. Track symptoms weekly rather than daily — hormonal shifts are slow, and daily tracking creates noise.
Amino acids also play an underappreciated role in hormone synthesis — how amino acid supplementation fits into broader metabolic health is worth understanding if fatigue and recovery are part of the picture alongside hormonal symptoms.
FAQs
Q. What vitamins help regulate hormones naturally?
The most effective vitamins and nutrients for hormone balance include:
- Vitamin D – supports hormone production and insulin sensitivity
- Vitamin B6 – helps regulate estrogen and progesterone balance
- Magnesium – reduces cortisol (stress hormone) and supports sleep
- Omega-3 fatty acids – lower inflammation and support hormonal signaling
- Zinc – essential for reproductive hormones and thyroid function
Targeted supplements:
- DIM (Diindolylmethane) – helps with estrogen metabolism
- Inositol – improves insulin sensitivity, especially in PCOS
These nutrients work best when combined with a balanced diet and a healthy lifestyle.
Q. How long does it take for vitamins to balance hormones?
- 4–8 weeks: Initial improvements (energy, mood, cycle regularity)
- 3–6 months: More noticeable hormonal rebalancing
Results depend on:
- Root cause of imbalance
- Consistency of supplement use
- Diet, sleep, and stress levels
Q. Can vitamins completely fix a hormonal imbalance?
Vitamins can significantly improve or support hormone balance, but they don’t always “fix” the issue completely.
Hormones are influenced by:
- Nutrition
- Sleep quality
- Stress levels
- Underlying conditions (like thyroid disorders or PCOS)
Supplements work within a system—not as a standalone solution.
Q. Do vitamins help with PCOS symptoms?
Yes, certain vitamins are especially helpful for PCOS (Polycystic Ovary Syndrome):
- Vitamin D – improves insulin resistance
- Magnesium – supports blood sugar control
- Inositol – directly targets insulin signaling and ovulation
These nutrients address root causes, not just symptoms, making them highly effective when used consistently.
Q. Can taking too many vitamins disrupt hormones?
Yes—over-supplementation can negatively affect hormone balance.
Common risks include:
- Excess fat-soluble vitamins (A, D, E, K) accumulate in the body
- High-dose Vitamin B6 causes nerve damage over time
- Too much Zinc leading to copper deficiency
More is not better. Always use supplements with a clear purpose and proper dosage.
Q. What is the fastest way to balance hormones naturally?
The most effective approach combines:
- Targeted supplementation (Vitamin D, magnesium, omega-3s, etc.)
- Low-glycaemic diet (to stabilize blood sugar)
- Consistent sleep routine (7–9 hours nightly)
- Stress management (exercise, mindfulness, reduced cortisol triggers)
No supplement works in isolation—and none work instantly. Sustainable habits drive real hormonal balance.
This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional before starting any new supplement regimen.
Explore our full library of expert-reviewed health and nutrition guides at Pure Magazine.